

Your front desk is busy. Providers are moving. Claims are sitting. Patient balances are creeping up. You open a spreadsheet at the end of the week and still can’t answer the one question that matters most: why is money taking so long to hit the bank account?
That’s where most small and mid-sized practices in Jacksonville get stuck. They’re not failing because they don’t work hard. They’re bleeding cash because the business side of medicine is fragmented. One person handles scheduling, another touches insurance verification, someone else codes, and nobody owns the full financial chain from appointment to payment.
That chain is healthcare revenue cycle management. If it’s weak, your cash flow gets erratic, denials pile up, compliance risk grows, and tax planning becomes harder because your books stop reflecting reality. You can’t make smart hiring, payroll, equipment, or quarterly tax decisions off bad timing and incomplete data.
Why Your Practice's Financial Health Depends on RCM
A clinic owner usually doesn’t call a CPA because things are calm. They call when accounts receivable is swelling, denials keep reappearing under different reason codes, and nobody trusts the month-end numbers.
That stress is predictable. Small and medium-sized healthcare practices have limited staff, limited time, and limited room for mistakes. At the same time, 61% of organizations plan RCM outsourcing, yet smaller firms often still lack practical guidance on cost-effective support like fractional CFO services or integrating QuickBooks with RCM workflows for compliance and year-end efficiency, according to DrChrono’s discussion of RCM challenges for smaller practices.
RCM is your financial heartbeat
Healthcare revenue cycle management is the full payment path. It starts when a patient schedules an appointment and ends when every legitimate dollar is collected, posted, reconciled, and reported correctly.
If you want a simple analogy, think of RCM like triage for your finances. You don’t ignore a patient’s vital signs and hope for the best. You also don’t ignore aging receivables, coding mistakes, underpayments, and weak patient collections and expect healthy cash flow.
Three things are always tied together:
- Cash flow: Delays in claims and collections starve the practice.
- Compliance: Sloppy processes increase billing and reporting risk.
- Decision-making: If your numbers are off, every tax and growth decision is weaker.
Why busy owners miss the real problem
Most owners focus on the visible fire. A rejected claim. A payer issue. A patient who didn’t pay. But the damage usually started earlier.
A missed eligibility check at scheduling can trigger a denial weeks later. Incomplete provider documentation can create coding errors. Delayed posting can make your reports look healthier or worse than they really are. Then tax planning, payroll timing, and vendor decisions all get made on distorted numbers.
Practical rule: If your billing team, bookkeeper, and tax preparer are all looking at different versions of the truth, your practice isn’t managing revenue. It’s reacting to it.
That’s why professional guidance isn’t optional. Software can process tasks. It can’t judge financial risk, spot process failure across departments, or translate messy RCM activity into clean books and sound business decisions.
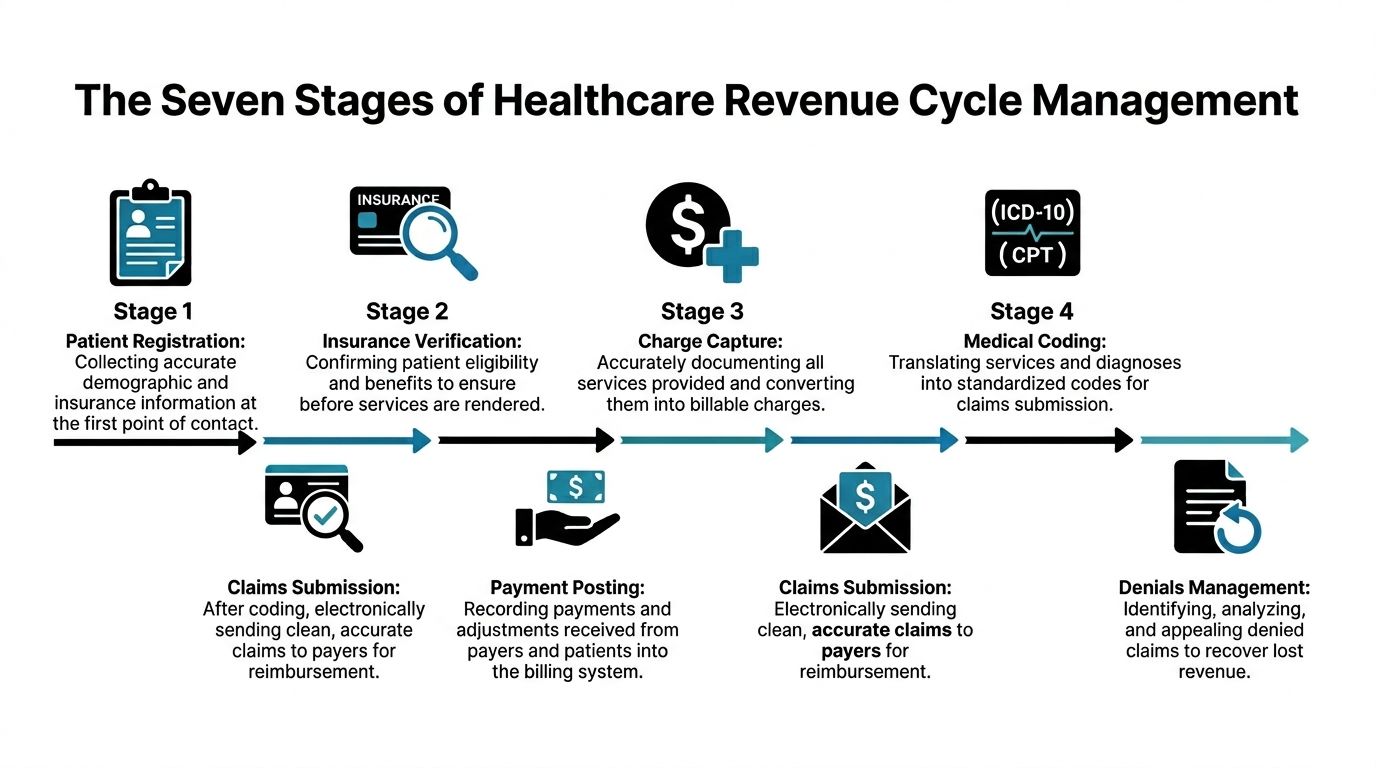
The Seven Stages of Healthcare Revenue Cycle Management
Healthcare revenue cycle management works like a relay race. If one runner fumbles the baton, the whole team loses time. In a clinic, the baton is accurate information and timely follow-through.
Pre-registration and scheduling
The race starts before the patient walks in.
Your staff collects demographics, payer details, referral information, and appointment data. If this step is rushed, every downstream step gets slower. A misspelled name, wrong insurance ID, or outdated address isn’t a front-desk problem. It becomes a payment problem.
Scheduling also shapes revenue timing. Empty slots hurt production. Overbooked schedules create rushed intake and more registration errors.
Patient registration and insurance verification
Many practices lose control at this stage.
You need active eligibility, benefit details, authorization requirements, and a clear patient responsibility estimate before service. If your team skips this or does it inconsistently, you’re approving work without confirming how it gets paid.
A lot of practices think they have an insurance issue. They have a process issue.
Verify first. Treat second. Bill third. That order protects cash flow.
Charge capture and medical coding
Now the clinical work has to become a billable financial event.
Charge capture means every service provided gets documented and translated into a charge. Coding means assigning the correct diagnosis and procedure codes to support the claim. If providers under-document, coders guess. If coders guess, denials and underpayments follow.
Revenue often leaks from this stage. Not always from fraud or big mistakes. Often from missed services, incomplete modifiers, or documentation that doesn’t support what was done.
Claims submission
A claim needs to be clean before it goes out. That means complete patient data, correct coding, proper payer rules, and all required supporting information.
Think of this like mailing a check to the wrong address with the wrong amount and expecting it to clear. Bad claims don’t just get denied. They also eat staff time because someone has to touch them again.
If your team needs a basic framework for the receivables side of this process, this overview of accounts receivable management is worth reviewing.
Payer adjudication and payment posting
Once the payer receives the claim, they process it according to the contract, coverage terms, and submitted documentation.
Your job doesn’t end when payment arrives. Payment posting must be accurate. Adjustments must be classified properly. Underpayments must be identified. If your staff posts money without reconciling against expected reimbursement, you can lose revenue and never see it.
This is one of the most overlooked parts of healthcare accounting. Many practices record deposits but don’t fully analyze what those deposits mean.
Patient billing and collections
After insurance, the patient balance remains.
This stage demands clarity. Patients pay faster when the statement is understandable, the estimate was explained early, and the practice offers practical payment methods. Patients don’t delay because they enjoy debt. They delay because the bill is confusing, late, or disconnected from what they expected.
A patient collections process has to be firm, professional, and easy to follow.
Denial management and reporting
Denials aren’t random bad luck. They’re feedback.
A denial should trigger three questions:
- What happened
- Why did it happen
- How do we stop it next time
Practices that only resubmit claims without tracking root causes stay trapped in rework. Strong denial management connects the denial back to the exact point of failure, whether that was registration, authorization, coding, charge entry, or payer follow-up.
Why the whole cycle must stay connected
The seven stages aren’t separate departments with separate goals. They are one financial system.
A practice owner should be able to trace revenue from appointment to bank deposit without guessing. If that sounds difficult in your office, your problem isn’t effort. It’s fragmented healthcare revenue cycle management.
Common Pitfalls That Cripple Practice Cash Flow
Cash flow usually doesn’t collapse because of one catastrophic event. It weakens through small operational mistakes that repeat every day.
The worst part is that these mistakes often look harmless in the moment. A rushed registration. A charge entered late. A denial left in a work queue because the team is short-staffed. Then the bank balance gets tighter and tighter.
The front-end errors that create back-end pain
Most receivable problems start before the claim is ever submitted.
Common revenue leaks include:
- Bad patient data: Wrong date of birth, old address, and inaccurate insurance details slow billing and create preventable denials.
- Weak eligibility checks: If coverage isn’t verified before service, the claim may fail later and turn into a patient balance that’s much harder to collect.
- Missing authorizations: Specialty and procedure-heavy practices get burned here all the time.
- Unclear patient estimates: Patients are less likely to pay promptly when the number surprises them.
These aren’t clerical issues. They are cash flow issues.
Coding and charge lag are expensive
Providers deliver care. Then the practice has to turn that care into a clean billable record. When documentation is incomplete or coding is rushed, reimbursement slows down.
Delayed charge entry is especially damaging. According to athenahealth’s medical revenue cycle guidance, a critical pitfall is allowing Days in Accounts Receivable to rise above the industry benchmark of 30 to 50 days. The same source notes that high-performing providers reduce A/R to 30 to 40 days through automation, which can enable 10 to 20% faster revenue realization.
That matters because time is money in a literal sense here. If charges sit unentered, claims don’t go out. If claims don’t go out, cash doesn’t come in.
Older A/R is like spoiled inventory. The longer it sits, the less likely you are to recover its full value.
Denials don’t fix themselves
Many practices treat denials as a normal cost of doing business. That’s the wrong mindset.
A denial is a signal that a process failed. If your team only works the denial itself and never addresses the root cause, you’re paying twice. Once in delayed cash flow, and again in labor spent reworking the account.
Here’s what weak denial management usually looks like:
| Revenue leak | What happens in practice | Financial effect |
|---|---|---|
| No denial categorization | Staff resubmits claims without pattern tracking | Same errors keep repeating |
| Slow follow-up | Claims age while staff handles current work | Cash receipts get delayed |
| No ownership | Billing, coding, and front desk each blame the other | Problems stay unresolved |
| Poor reporting | Owner sees total A/R but not the reason behind it | Decisions get made blindly |
Reporting gaps make everything worse
A lot of owners see monthly revenue and think they understand the business. They don’t.
You need to know whether cash came in because the practice is operating well or because staff finally cleaned up old claims. You need to know whether collections are healthy or whether receivables are aging behind the scenes.
If your books don’t tie operational billing activity to financial reporting, you can’t manage staffing, taxes, partner distributions, or growth with confidence. You’re driving with a fogged windshield.
Key RCM Metrics You Must Track for Financial Health
If you don’t track the right metrics, you’ll manage the practice by mood. That’s a bad way to run a medical business.
The healthcare industry already has a framework for this. The HFMA MAP Keys include 29 KPIs across five categories, and two of the most important for smaller practices are Net Collection Rate above 95% and Days in A/R ideally at or below 30 to 40 days.

Net collection rate
Net Collection Rate, or NCR, tells you how much collectible revenue you collected after contractual adjustments.
The formula is straightforward:
Payments collected / (Charges – Contractual adjustments) x 100
A strong target is above the benchmark already noted in the HFMA standard. If your number is lagging, the practice is likely losing money through underpayments, denials, bad follow-up, or write-offs that shouldn’t be happening.
NCR is one of the fastest ways to tell whether the practice gets paid what it has earned.
Days in accounts receivable
This metric shows how long it takes to convert billed revenue into cash.
When A/R days climb, your liquidity gets squeezed. Payroll, supplies, tax payments, and owner draws all get tighter because your money is trapped in process instead of sitting in the operating account.
Owners who want a better grasp of related receivables analysis should understand the accounts receivable turnover ratio because it helps connect collections efficiency to broader financial reporting.
Clean claims rate and cost to collect
The medical finance literature also points to clean claims rate and cost to collect as core healthcare revenue cycle management indicators in day-to-day practice operations, as discussed in this NCBI overview of healthcare finance and RCM drivers.
Use them this way:
- Clean claims rate: This tells you whether claims go out correctly the first time. If it’s weak, look upstream at registration, eligibility, documentation, and coding.
- Cost to collect: This tells you how much the practice spends to collect revenue. If labor and vendor costs rise while collections stay messy, your process is too expensive.
- Charge capture: This helps expose services that were performed but not billed.
- Patient pay yield: This shows how effectively the practice collects from patients.
Here’s a quick visual explainer before you audit your dashboard:
What these numbers should trigger
Don’t just look at a dashboard and move on. Tie each metric to an action.
- Low NCR: Audit denials, underpayments, and write-off approvals.
- High Days in A/R: Review charge lag, insurance verification, and follow-up speed.
- Poor clean claims rate: Check front-end accuracy and coding workflow.
- High cost to collect: Reassess staffing, tools, and handoffs between systems.
Diagnostic view: Metrics are your MRI. They don’t fix the problem, but they show exactly where the financial injury is.
A Step-by-Step Plan to Optimize Your RCM
A good RCM process is disciplined, not magical. You don’t need more chaos, more spreadsheets, or another software demo. You need a tighter operating system.
The goal is simple. Collect the right money, faster, with less rework and fewer compliance mistakes.
Start at the front desk
If your intake process is sloppy, the rest of the cycle never recovers.
Put strict controls in place:
- Standardize registration fields: Don’t let staff skip required demographic and payer information.
- Verify eligibility before every visit: Not once a year. Every visit.
- Confirm authorizations before service: Especially in specialties and higher-dollar encounters.
- Communicate patient responsibility early: Patients pay better when the amount is explained before the visit, not after a confusing statement arrives.
This is basic blocking and tackling. It’s not glamorous. It works.
Tighten charge capture and coding discipline
Providers should document completely and promptly. Coders should work from clear records, not assumptions. Charge entry should happen fast enough that claims don’t stall in limbo.
Review workflow for these weak spots:
- Delayed sign-offs by providers
- Missed ancillary services
- Coding edits that keep repeating
- Lack of periodic chart and coding review
A small clinic doesn’t need a giant compliance department. It does need a documented process and someone accountable for checking whether the process is followed.
Build a denial process that attacks root cause
You want fewer denials, not just more resubmissions.
According to Global Healthcare Resource’s KPI discussion, a key optimization goal is NCR above 95%. That source also notes that top performers reach 98% NCR through root-cause denial analysis, appealing over 65% of denials, and using digital patient portals that can improve point-of-service collections by 20 to 30%.
That tells you exactly where to focus:
- Categorize denials: Eligibility, authorization, coding, medical necessity, timely filing, and underpayment should not live in one vague bucket.
- Assign ownership: Front desk owns registration accuracy. Clinical staff own documentation quality. Billing owns timely submission and follow-up.
- Appeal intelligently: Don’t appeal everything blindly. Appeal what is collectible and document why it happened.
- Report patterns monthly: One denial is a task. Repeated denials are a management issue.
Make patient collections easier, not softer
Small practices often avoid direct financial conversations because they don’t want to upset patients. That hesitation costs money.
You can be respectful and firm at the same time.
A practical patient-pay approach includes:
- Clear estimates before service
- Point-of-service collection attempts
- Digital payment options
- Structured payment plans for appropriate balances
- Statements that humans can understand
If you want a broader outside perspective on collection discipline, these accounts receivable best practices are useful because the underlying habits apply well to healthcare billing too.
Clean up the accounting side
This is the part many owners ignore. Billing data without clean accounting is half a system.
You need the general ledger, deposit posting, A/R reporting, write-offs, refunds, payroll, and tax planning to align. Otherwise, the practice might look profitable on paper while cash flow remains unstable. Or worse, owners may over-distribute based on distorted numbers and create tax and liquidity problems later.
Treat tax and compliance as part of RCM
Tax law changes, payroll obligations, entity structure questions, and reimbursement reporting don’t sit in a separate universe. They are connected to how revenue is recorded and when cash is received.
When revenue timing is messy:
- estimated tax planning gets weaker
- compensation decisions get riskier
- year-end cleanup gets more expensive
- compliance errors become easier to miss
That’s why a fractional CFO mindset matters. Someone has to connect operations, reporting, taxes, and strategy. If nobody owns that view, the practice keeps running hard without getting financially sharper.
In-House RCM vs Outsourcing with a CPA Firm
Some owners want complete internal control. I understand that. Handing off part of your revenue cycle can feel risky.
But keeping everything in-house isn’t the same as being in control. If your team is overextended, undertrained, or disconnected from the accounting and tax side, you don’t have control. You have dependency on a fragile process.
What the market is signaling
Healthcare leaders are already responding to pressure. Undue Medical Debt’s revenue cycle perspective notes that 67% of healthcare executives report rising claim denials and 63% are increasing outsourcing. The same source also makes an important point for smaller Florida practices: a hybrid model with a local CPA can offer a better balance by preserving oversight while improving compliance and helping owners manage AI tools and regulatory change.
That hybrid point is the main takeaway.
A side-by-side comparison
| Factor | In-House RCM | Outsourced to CPA Firm |
|---|---|---|
| Daily control | Staff is on site and visible | Control shifts to process oversight and reporting |
| Expertise depth | Depends on who you can hire and retain | Broader accounting, compliance, tax, and financial analysis support |
| Compliance risk | Can rise if staff wears too many hats | Stronger review discipline and outside oversight |
| Technology use | Often tied to current software and staff habits | More likely to include workflow review, reporting structure, and integration advice |
| Scalability | Hiring and training become bottlenecks | Easier to expand support without adding full-time overhead |
| Owner visibility | Can be murky if reports are inconsistent | Often stronger when KPI reporting ties to financial statements |
Where in-house works
An internal team can work well if your practice has:
- Experienced billing leadership
- Reliable coding support
- Strong reporting discipline
- Tight coordination between billing and accounting
If those pieces are in place, keeping more functions internal can preserve familiarity and immediate communication.
But many small and midsize practices don’t have all of that. They have one or two strong employees carrying too much. That’s not a system. That’s a vulnerability.
Why a CPA-led model is different from a billing vendor
A billing vendor usually focuses on transactions. A CPA-led partnership should focus on the full financial picture.
That means:
- receivables management
- reconciliation
- write-off review
- cash flow visibility
- compliance support
- payroll and tax alignment
- fractional CFO guidance for decisions, not just data entry
That broader view matters in Florida practices because business owners are juggling state-specific operating realities, payer complexity, federal tax obligations, payroll filings, and increasing automation tools. If you adopt AI or workflow software without understanding oversight and reporting requirements, you can create a new mess faster than you solve the old one.
If you want to evaluate what a specialized partner should cover, review this page on healthcare accounting services.bookkeepingandaccountinginc.com/our-services-healthcare-accounting/). It gives a good benchmark for the range of support a practice should expect beyond plain bookkeeping.
A good CPA partner doesn’t replace your team. They give your team guardrails, better reporting, and financial leadership.
My recommendation for Jacksonville practices
For most small and medium-sized clinics, the best model is not pure in-house and not blind outsourcing. It’s a hybrid.
Keep patient-facing functions and daily operational touchpoints close to the practice. Layer in outside CPA and fractional CFO support for oversight, reconciliations, compliance, KPI review, tax planning, and process correction.
That structure gives you three things owners usually want at the same time:
- Visibility
- Accountability
- Better decisions
Without that mix, owners often get one of two bad outcomes. Either they overpay for fragmented internal labor, or they outsource too much and lose sight of what’s happening inside their own business.
Your Northeast Florida RCM Compliance Checklist
If you run a Jacksonville-area practice, use this as a real operating checklist. Not a nice idea. A checklist.
Weekly and monthly checks that matter
- Verify insurance before service: Confirm eligibility and benefits for every scheduled patient, not just new ones.
- Review A/R aging weekly: Focus on old balances first, especially claims and patient accounts that are lingering without action.
- Check charge lag: Make sure services move from encounter to billable claim quickly.
- Audit denial reasons: Don’t accept “denied” as an answer. Track why.
- Reconcile payment posting: Match posted payments and adjustments to expected reimbursement logic.
- Watch patient balances: If statements are confusing, collections will suffer.
Compliance and reporting discipline
- Quarterly coding review: Look at frequently used CPT and diagnosis patterns for consistency and support.
- Monitor write-offs: Require approval and documentation. Casual write-offs hide process problems.
- Tie RCM to bookkeeping: Deposits, receivables, refunds, and contractual adjustments should line up with financial reporting.
- Review tax planning against actual cash flow: Don’t make estimated tax decisions from stale numbers.
- Train staff when tools change: New software, AI features, and workflow automation need oversight.
If your practice is evaluating automation, voice tools, or workflow bots, this guide to understanding the regulatory environment for healthcare AI is a useful read. Technology can help, but only if your compliance habits are stronger than your enthusiasm.
What owners should ask themselves
Use these questions as a final gut check:
- Can I explain why my cash is where it is today
- Do I know my biggest denial pattern
- Do my books reflect billing reality
- Am I making payroll, tax, and growth decisions from timely financials
- Do I have expert guidance, or just software and hope
Healthcare revenue cycle management is too important to leave scattered across front desk habits, billing shortcuts, and year-end cleanup. In Northeast Florida, where small practices have to stay lean and compliant at the same time, local financial guidance is not a luxury. It’s part of operating responsibly.
Bookkeeping and Accounting of Florida Inc. helps Jacksonville and Northeast Florida healthcare practices bring order to messy revenue cycles with clean books, compliance support, tax guidance, and fractional CFO insight. If your practice needs clearer cash flow, stronger reporting, and a CPA team that understands healthcare accounting, visit Bookkeeping and Accounting of Florida Inc. and schedule a consultation.
